The Truth About Over-Pronation Of The Feet
Overview
Pronation describes the natural process of the inward rolling of your foot when the outer edge of your heel strikes the ground and your foot flattens out. Excess pronation, known as flat foot, can result in flattened arches and overstretched foot muscles. Advanced conditions may affect your hips, knees, ankle, back and foot functioning. Use natural techniques to stretch and strengthen your muscles in order to help pronation.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Because overpronation affects the entire lower leg, many injuries and conditions may develop and eventually cause problems not only in the leg and foot, but also the knee, hips and lower back. Pain often begins in the arch of the foot or the ankle. Blisters may develop on the instep, or on the inside edge of the heels. As overpronation continues and problems develop, pain will be felt elsewhere, depending on the injury.
Diagnosis
Do the wet foot test. Get your feet wet and walk along a paved surface or sand and look at the footprints you leave. If you have neutral feet you will see a print of the heel with a thin strip connecting to your forefoot, but if you're overpronating your foot print will look a bit like a giant blob with toes.
Non Surgical Treatment
Side Step with Opposite Reach. This exercise is designed to load the "bungee cord system" of the gluteal muscle and its opposite, latissimus dorsi muscle to keep the foot from overpronating. Because the opposite arm swings across the front leg when walking, this exercise creates tension in the muscles all the way from the front foot, across the back of the hips and back, to the fingers of the opposite hand. Movement Directions. Stand with left foot on top of the dome of the BT. (Note: For added balance, the right foot can tap on the ground, if needed). Reach right leg out to the side of the BT, and tap the ground while squatting down on the left side and reaching right arm across the left knee. Push down with left big toe while squatting. This activates the arch of the left foot and strengthens all the stabilizing muscles on the left side of the lower body. Return to starting position. Perform 8 to 10 repetitions on each leg.
Surgical Treatment
Subtalar Arthroereisis. The ankle and hindfoot bones/midfoot bones around the joint are fused, locking the bones in place and preventing all joint motion. This may also be done in combination with fusion at other joints. This is a very aggressive option usually reserved for extreme cases where no joint flexibility is present and/or the patient has severe arthritic changes in the joint.
Pronation describes the natural process of the inward rolling of your foot when the outer edge of your heel strikes the ground and your foot flattens out. Excess pronation, known as flat foot, can result in flattened arches and overstretched foot muscles. Advanced conditions may affect your hips, knees, ankle, back and foot functioning. Use natural techniques to stretch and strengthen your muscles in order to help pronation.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Because overpronation affects the entire lower leg, many injuries and conditions may develop and eventually cause problems not only in the leg and foot, but also the knee, hips and lower back. Pain often begins in the arch of the foot or the ankle. Blisters may develop on the instep, or on the inside edge of the heels. As overpronation continues and problems develop, pain will be felt elsewhere, depending on the injury.
Diagnosis
Do the wet foot test. Get your feet wet and walk along a paved surface or sand and look at the footprints you leave. If you have neutral feet you will see a print of the heel with a thin strip connecting to your forefoot, but if you're overpronating your foot print will look a bit like a giant blob with toes.
Non Surgical Treatment
Side Step with Opposite Reach. This exercise is designed to load the "bungee cord system" of the gluteal muscle and its opposite, latissimus dorsi muscle to keep the foot from overpronating. Because the opposite arm swings across the front leg when walking, this exercise creates tension in the muscles all the way from the front foot, across the back of the hips and back, to the fingers of the opposite hand. Movement Directions. Stand with left foot on top of the dome of the BT. (Note: For added balance, the right foot can tap on the ground, if needed). Reach right leg out to the side of the BT, and tap the ground while squatting down on the left side and reaching right arm across the left knee. Push down with left big toe while squatting. This activates the arch of the left foot and strengthens all the stabilizing muscles on the left side of the lower body. Return to starting position. Perform 8 to 10 repetitions on each leg.
Surgical Treatment
Subtalar Arthroereisis. The ankle and hindfoot bones/midfoot bones around the joint are fused, locking the bones in place and preventing all joint motion. This may also be done in combination with fusion at other joints. This is a very aggressive option usually reserved for extreme cases where no joint flexibility is present and/or the patient has severe arthritic changes in the joint.
How To Get Rid Of Bunions On Feet
Overview
 A bunion (hallux abducto valgus) is a bony lump or enlargement that forms in the joint (metatarsal phalangeal joint) at the base of the big toe. The big toe points toward the other toes (lateral deviation) as the bunion progresses. The joint and surrounding tissue becomes inflamed and painful. Occasionally bunions can also form at the joint at the base of the smallest (fifth) toe. They are called a tailor's bunion or bunionette. Bunions can be accompanied by bursitis (inflammation of a small fluid-filled sac adjacent to the joint). With an advanced bunion the big toe may be so deformed that it has to lie over or under the second toe. In this situation it hurts to walk or wear any kind of shoe. About one in three people in most Western countries will get a bunion. They are about ten times more common in women than in men. Older people are more often affected than younger people, although bunions do occur in children with misaligned feet. Bunions should not be confused with gout or arthritis, which can also cause inflammation, deformity and pain around the toes and feet.
A bunion (hallux abducto valgus) is a bony lump or enlargement that forms in the joint (metatarsal phalangeal joint) at the base of the big toe. The big toe points toward the other toes (lateral deviation) as the bunion progresses. The joint and surrounding tissue becomes inflamed and painful. Occasionally bunions can also form at the joint at the base of the smallest (fifth) toe. They are called a tailor's bunion or bunionette. Bunions can be accompanied by bursitis (inflammation of a small fluid-filled sac adjacent to the joint). With an advanced bunion the big toe may be so deformed that it has to lie over or under the second toe. In this situation it hurts to walk or wear any kind of shoe. About one in three people in most Western countries will get a bunion. They are about ten times more common in women than in men. Older people are more often affected than younger people, although bunions do occur in children with misaligned feet. Bunions should not be confused with gout or arthritis, which can also cause inflammation, deformity and pain around the toes and feet.
Causes
The commonest cause of bunions is prolonged wearing of poorly designed shoes such as the narrow high heels that women wear. This is one of the reasons why bunions are much more common in women than in men. There is also a hereditary component to bunions in that many times we will see a grandmother, mother and daughter all with various stages of bunions. 38% of women in the United States wear shoes that are too small and 55% of women have some degree of bunion formation. Bunions are 9 times more common in women than they are in men.
Symptoms
Symptoms include redness, swelling and pain which may be present along the inside margin of the foot. The patients feet may become too wide to fit into their normal size shoes and moderate to severe discomfort may occur when the patient is wearing tight shoes. A "hammer toe" may occur at the 2nd toe. This is when the toe contracts and presses on the shoe. Subsequently, this may cause a corn on top of the 2nd toe.
Diagnosis
When an x-ray of a bunion is taken, there is usually angulation between the first metatarsal bone and the bones of the big toe. There may also be angulation between the first and second metatarsal bones. These angular irregularities are the essence of most bunions. In general, surgery for bunions aims to correct such angular deformities.
Non Surgical Treatment
Your podiatrist can recommend exercises, orthoses (special devices inserted into shoes), shoe alterations or night splints (which hold toes straight over night) which may slow the progression of bunions in children. According to experts, ?conservative? measures such as these may help relieve symptoms, though there is no evidence they can correct the underlying deformity. Orthoses are designed to prevent the problem getting worse by decreasing any biomechanical causes of bunions. In other words, if the biomechanical theory is correct (i.e. if your bunions are caused by the way you walk), orthoses may help you walk in a way that doesn?t exacerbate the problem. But it won?t change the already established shape of your foot. For that, you need surgery. 
Surgical Treatment
Depending on the size of the enlargement, misalignment of the toe, and pain experienced, conservative treatments may not be adequate to prevent progressive damage from bunions. In these cases, bunion surgery, known as a bunionectomy, may be advised to remove the bunion and realign the toe.
Prevention
Choosing footwear that fits correctly, especially low heeled shoes with plenty of space for the toes, is one of the main ways that bunions can be prevented. Always stand when trying on shoes to ensure they still fit comfortably when the foot expands under your body weight. Try shoes on both feet, and select the size appropriate for your larger foot. Use an extra insole if one shoe is looser than the other. Do not cramp the larger foot. People prone to flat-footedness should consider the use of arch supports, orthotic shoe inserts or special orthotic shoes to prevent or delay the development of bunions.
Coping With Severs Disease
Overview
Sever's disease is the most common cause of heel pain in the growing child. It is due to overuse and repetitive stress of the Achilles tendon where it attaches to the heel bone.
Causes
The condition generally occurs in active children at early adolescence during rapid growth periods as the heel bone can grow faster than the leg muscles causing them to become tight and overstretched. Sever?s disease most often caused by inadequate footwear, playing sport on hard surfaces, calf tightness and biomechanical problems.
Symptoms
Severs causes swelling, pain and tenderness over the back of the heel. Your child may walk with a limp. Initially the pain may be intermittent occurring only during or after exercise. As the problem gets worse, pain may be present most of the time. The swelling increases and is painful when touched or knocked. It commonly affects boys who are having a growth spurt during their pre-teen or teenage years. One or both knees may be affected.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
Initially, treatment will consist of resting from activity, ice and anti-inflammatory medications to reduce the pain. Your physiotherapist may also use a variety of pain reducing techniques such as soft tissue massage or joint mobilisations. They may recommend taping to unload the area of pain, heel cups or wedge inserts into the bottom of your shoe. Also in the initial phase we may also refer you to podiatry for orthotics and/or further footwear recommendations. It is also ideal in the first instance to start stretching your calf muscles and achilles. This initial phase typically lasts for 1-2 weeks. During this time your physiotherapist will guide you on appropriate levels of activity- they may recommend you rest from impact type activities during this phase, and will guide you on the best program to return to your sport without any further injury.
Recovery
One of the most important things to know about Sever's disease is that, with proper care, the condition usually goes away within 2 weeks to 2 months and does not cause any problems later in life. The sooner Sever's disease is addressed, the quicker recovery is. Most kids can return to physical activity without any trouble once the pain and other symptoms go away. Although Sever's disease generally heals quickly, it can recur if long-term measures are not taken to protect the heel during a child's growing years. One of the most important is to make sure that kids wear proper shoes. Good quality, well-fitting shoes with shock-absorbent (padded) soles help to reduce pressure on the heel. The doctor may also recommend shoes with open backs, such as sandals or clogs, that do not rub on the back of the heel. Shoes that are heavy or have high heels should be avoided. Other preventive measures include continued stretching exercises and icing of the affected heel after activity.
Sever's disease is the most common cause of heel pain in the growing child. It is due to overuse and repetitive stress of the Achilles tendon where it attaches to the heel bone.
Causes
The condition generally occurs in active children at early adolescence during rapid growth periods as the heel bone can grow faster than the leg muscles causing them to become tight and overstretched. Sever?s disease most often caused by inadequate footwear, playing sport on hard surfaces, calf tightness and biomechanical problems.
Symptoms
Severs causes swelling, pain and tenderness over the back of the heel. Your child may walk with a limp. Initially the pain may be intermittent occurring only during or after exercise. As the problem gets worse, pain may be present most of the time. The swelling increases and is painful when touched or knocked. It commonly affects boys who are having a growth spurt during their pre-teen or teenage years. One or both knees may be affected.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
Initially, treatment will consist of resting from activity, ice and anti-inflammatory medications to reduce the pain. Your physiotherapist may also use a variety of pain reducing techniques such as soft tissue massage or joint mobilisations. They may recommend taping to unload the area of pain, heel cups or wedge inserts into the bottom of your shoe. Also in the initial phase we may also refer you to podiatry for orthotics and/or further footwear recommendations. It is also ideal in the first instance to start stretching your calf muscles and achilles. This initial phase typically lasts for 1-2 weeks. During this time your physiotherapist will guide you on appropriate levels of activity- they may recommend you rest from impact type activities during this phase, and will guide you on the best program to return to your sport without any further injury.
Recovery
One of the most important things to know about Sever's disease is that, with proper care, the condition usually goes away within 2 weeks to 2 months and does not cause any problems later in life. The sooner Sever's disease is addressed, the quicker recovery is. Most kids can return to physical activity without any trouble once the pain and other symptoms go away. Although Sever's disease generally heals quickly, it can recur if long-term measures are not taken to protect the heel during a child's growing years. One of the most important is to make sure that kids wear proper shoes. Good quality, well-fitting shoes with shock-absorbent (padded) soles help to reduce pressure on the heel. The doctor may also recommend shoes with open backs, such as sandals or clogs, that do not rub on the back of the heel. Shoes that are heavy or have high heels should be avoided. Other preventive measures include continued stretching exercises and icing of the affected heel after activity.
Flat Foot Symptoms In Adults
Overview
Originally known as posterior tibial tendon dysfunction or insufficiency, adult-acquired flatfoot deformity encompasses a wide range of deformities. These deformities vary in location, severity, and rate of progression. Establishing a diagnosis as early as possible is one of the most important factors in treatment. Prompt early, aggressive nonsurgical management is important. A patient in whom such treatment fails should strongly consider surgical correction to avoid worsening of the deformity. In all four stages of deformity, the goal of surgery is to achieve proper alignment and maintain as much flexibility as possible in the foot and ankle complex. However, controversy remains as to how to manage flexible deformities, especially those that are severe. 
Causes
Flat feet causes greater pressure on the posterior tibial tendon than normal. As the person with flat feet ages, the muscles, tendons and ligaments weaken. Blood supplies diminish as arteries narrow. These conditions are magnified for obese patients because of their increased weight and atherosclerosis. Finally, the tendon gives out or tears. Most of the time, this is a slow process. Once the posterior tibial tendon and ligaments stretch, body weight causes the bones of the arch to move out of position. The foot rotates inward (pronation), the heel bone is tilted to the inside, and the arch appears collapsed. In some cases, the deformity progresses until the foot dislocates outward from the ankle joint.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms here. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
Diagnostic testing is often used to diagnose the condition and help determine the stage of the disease. The most common test done in the office setting are weightbearing X-rays of the foot and ankle. These assess joint alignment and osteoarthritis. If tendon tearing or rupture is suspected, the gold standard test would be MRI. The MRI is used to check the tendon, surrounding ligament structures and the midfoot and hindfoot joints. An MRI is essential if surgery is being considered.
Non surgical Treatment
Nonoperative treatment of posterior tibial tendon dysfunction can be successful with the Arizona AFO brace, particularly when treatment is initiated in the early stages of the disease. This mandates that the orthopedist has a high index of suspicion when evaluating patients to make an accurate diagnosis. Although there is a role for surgical management of acquired flat feet, a well-fitted, custom-molded leather and polypropylene orthosis can be effective at relieving symptoms and either obviating or delaying any surgical intervention. In today's climate of patient satisfaction directed health care, a less invasive treatment modality that relieves pain may prove to be more valuable than similar pain relief that is obtained after surgery. Questions regarding the long-term results of bracing remain unanswered. Future studies are needed to determine if disease progression and arthrosis occur despite symptomatic relief with a brace. Furthermore, age- and disease stage-matched control groups who are randomized to undergo surgery or bracing are necessary to compare these different treatment modalities. 
Surgical Treatment
If conservative treatments don?t work, your doctor may recommend surgery. Several procedures can be used to treat posterior tibial tendon dysfunction; often more than one procedure is performed at the same time. Your doctor will recommend a specific course of treatment based on your individual case. Surgical options include. Tenosynovectomy. In this procedure, the surgeon will clean away (debride) and remove (excise) any inflamed tissue surrounding the tendon. Osteotomy. This procedure changes the alignment of the heel bone (calcaneus). The surgeon may sometimes have to remove a portion of the bone. Tendon transfer: This procedure uses some fibers from another tendon (the flexor digitorum longus, which helps bend the toes) to repair the damaged posterior tibial tendon. Lateral column lengthening, In this procedure, the surgeon places a small wedge-shaped piece of bone into the outside of the calcaneus. This helps realign the bones and recreates the arch. Arthrodesis. This procedure welds (fuses) one or more bones together, eliminating movement in the joint. This stabilizes the hindfoot and prevents the condition from progressing further.
Dealing With Achilles Tendinitis
Overview
 Achilles tendinitis (tendonitis) or Achilles tendon inflammation occurs when the Achilles tendon becomes inflamed, as a result, of the Achilles tendon being put under too much strain. The Achilles tendon joins the calf muscles to the heel bone, and is found at the back of a person's lower leg. It is the largest tendon in the body and can endure great force, but is still susceptible to injury. Achilles tendinitis is usually the result of strenuous, high impact exercise, such as running. If ignored, Achilles tendinitis can lead to the tendon tearing or rupturing, and therefore it is important to seek the necessary treatment. Sometimes, treatment can be as simple as getting rest or changing an exercise routine. However, in more severe cases, surgery may be required.
Achilles tendinitis (tendonitis) or Achilles tendon inflammation occurs when the Achilles tendon becomes inflamed, as a result, of the Achilles tendon being put under too much strain. The Achilles tendon joins the calf muscles to the heel bone, and is found at the back of a person's lower leg. It is the largest tendon in the body and can endure great force, but is still susceptible to injury. Achilles tendinitis is usually the result of strenuous, high impact exercise, such as running. If ignored, Achilles tendinitis can lead to the tendon tearing or rupturing, and therefore it is important to seek the necessary treatment. Sometimes, treatment can be as simple as getting rest or changing an exercise routine. However, in more severe cases, surgery may be required.
Causes
Achilles tendonitis is an overuse injury that is common especially to joggers and jumpers, due to the repetitive action and so may occur in other activities that requires the same repetitive action. Most tendon injuries are the result of gradual wear and tear to the tendon from overuse or ageing. Anyone can have a tendon injury, but people who make the same motions over and over in their jobs, sports, or daily activities are more likely to damage a tendon. A tendon injury can happen suddenly or little by little. You are more likely to have a sudden injury if the tendon has been weakened over time. Common causes of Achilles tendonitis include, over-training or unaccustomed use,?too much too soon?. Sudden change in training surface e.g. grass to bitumen. Flat (over-pronated) feet, High foot arch with tight Achilles tendon. tight hamstring (back of thigh) and calf muscles, toe walking (or constantly wearing high heels). Poorly supportive footwear, hill running. Poor eccentric strength.
Symptoms
Symptoms of acute achilles tendonitis will be a gradual onset of achilles pain at the back of the ankle, just above the heel bone. This may develop over a period of days. The achilles tendon may be painful and stiff at the start of exercise and first thing in the morning. As the tendon warms up the pain will go often for it to return later in the day or towards the end of a prolonged training session. The tendon will be very tender on palpation or pressing in on the achilles tendon or squeezing it from the sides. Chronic achilles tendonitis may follow on from acute achilles tendonitis if it goes untreated or is not allowed sufficient rest. Chronic achilles tendonitis is a difficult condition to treat, particularly in older athletes who appear to suffer more often.
Diagnosis
A podiatrist can usually make the diagnosis by clinical history and physical examination alone. Pain with touching or stretching the tendon is typical. There may also be a visible swelling to the tendon. The patient frequently has difficulty plantarflexing (pushing down the ball of the foot and toes, like one would press on a gas pedal), particularly against resistance. In most cases X-rays don't show much, as they tend to show bone more than soft tissues. But X-rays may show associated degeneration of the heel bone that is common with Achilles Tendon problems. For example, heel spurs, calcification within the tendon, avulsion fractures, periostitis (a bruising of the outer covering of the bone) may all be seen on X-ray. In cases where we are uncertain as to the extent of the damage to the tendon, though, an MRI scan may be necessary, which images the soft tissues better than X-rays. When the tendon is simply inflamed and not severely damaged, the problem may or may not be visible on MRI. It depends upon the severity of the condition.
Nonsurgical Treatment
Many physical therapies exist to help with the pain. We have found the combination of modalities, stretching, acupuncture, footwear modification and myofascial release to be very effective. In resilient cases, a promising new treatment called Radial Shockwave may be indicated. The key to the treatment of this, and other foot problems, is an accurate diagnosis. With this, a treatment regimen tailored to you and your specific situation can be devised. We treat many acute and chronic achilles tendinitis in Edmonton and St. Albert, so remember ?it shouldn?t hurt.?

Surgical Treatment
Following the MRI or ultrasound scan of the Achilles tendon the extent of the degenerative change would have been defined. The two main types of operation for Achilles tendinosis are either a stripping of the outer sheath (paratenon) and longitudinal incisions into the tendon (known as a debridement) or a major excision of large portions of the tendon, the defects thus created then being reconstructed using either allograft (donor tendon, such as Wright medical graft jacket) or more commonly using a flexor hallucis longus tendon transfer. In cases of Achilles tendonosis with more minor degrees of degenerative change the areas can be stimulated to repair itself by incising the tendon, in the line of the fibres, which stimulates an ingrowth of blood vessels and results in the healing response. With severe Achilles tendonosis, occasionally a large area of painful tendon needs to be excised which then produces a defect which requires filling. This is best done by transferring the flexor hallucis longus muscle belly and tendon, which lies adjacent to the Achilles tendon. This results in a composite/double tendon after the operation, with little deficit from the transferred tendon.
Prevention
Stay in good shape year-round and try to keep your muscles as strong as they can be. Strong, flexible muscles work more efficiently and put less stress on your tendon. Increase the intensity and length of your exercise sessions gradually. This is especially important if you've been inactive for a while or you're new to a sport. Always warm up before you go for a run or play a sport. If your muscles are tight, your Achilles tendons have to work harder to compensate. Stretch it out. Stretch your legs, especially your calves, hamstrings, quadriceps, and thigh muscles - these muscles help stabilize your knee while running. Get shoes that fit properly and are designed for your sport. If you're a jogger, go to a running specialty store and have a trained professional help you select shoes that match your foot type and offer plenty of support. Replace your shoes before they become worn out. Try to run on softer surfaces like grass, dirt trails, or synthetic tracks. Hard surfaces like concrete or asphalt can put extra pressure on the joints. Also avoid running up or down hills as much as possible. Vary your exercise routine. Work different muscle groups to keep yourself in good overall shape and keep individual muscles from getting overused. If you notice any symptoms of Achilles tendonitis, stop running or doing activities that put stress on your feet. Wait until all the pain is gone or you have been cleared to start participating again by a doctor.
Achilles tendinitis (tendonitis) or Achilles tendon inflammation occurs when the Achilles tendon becomes inflamed, as a result, of the Achilles tendon being put under too much strain. The Achilles tendon joins the calf muscles to the heel bone, and is found at the back of a person's lower leg. It is the largest tendon in the body and can endure great force, but is still susceptible to injury. Achilles tendinitis is usually the result of strenuous, high impact exercise, such as running. If ignored, Achilles tendinitis can lead to the tendon tearing or rupturing, and therefore it is important to seek the necessary treatment. Sometimes, treatment can be as simple as getting rest or changing an exercise routine. However, in more severe cases, surgery may be required.
Causes
Achilles tendonitis is an overuse injury that is common especially to joggers and jumpers, due to the repetitive action and so may occur in other activities that requires the same repetitive action. Most tendon injuries are the result of gradual wear and tear to the tendon from overuse or ageing. Anyone can have a tendon injury, but people who make the same motions over and over in their jobs, sports, or daily activities are more likely to damage a tendon. A tendon injury can happen suddenly or little by little. You are more likely to have a sudden injury if the tendon has been weakened over time. Common causes of Achilles tendonitis include, over-training or unaccustomed use,?too much too soon?. Sudden change in training surface e.g. grass to bitumen. Flat (over-pronated) feet, High foot arch with tight Achilles tendon. tight hamstring (back of thigh) and calf muscles, toe walking (or constantly wearing high heels). Poorly supportive footwear, hill running. Poor eccentric strength.
Symptoms
Symptoms of acute achilles tendonitis will be a gradual onset of achilles pain at the back of the ankle, just above the heel bone. This may develop over a period of days. The achilles tendon may be painful and stiff at the start of exercise and first thing in the morning. As the tendon warms up the pain will go often for it to return later in the day or towards the end of a prolonged training session. The tendon will be very tender on palpation or pressing in on the achilles tendon or squeezing it from the sides. Chronic achilles tendonitis may follow on from acute achilles tendonitis if it goes untreated or is not allowed sufficient rest. Chronic achilles tendonitis is a difficult condition to treat, particularly in older athletes who appear to suffer more often.
Diagnosis
A podiatrist can usually make the diagnosis by clinical history and physical examination alone. Pain with touching or stretching the tendon is typical. There may also be a visible swelling to the tendon. The patient frequently has difficulty plantarflexing (pushing down the ball of the foot and toes, like one would press on a gas pedal), particularly against resistance. In most cases X-rays don't show much, as they tend to show bone more than soft tissues. But X-rays may show associated degeneration of the heel bone that is common with Achilles Tendon problems. For example, heel spurs, calcification within the tendon, avulsion fractures, periostitis (a bruising of the outer covering of the bone) may all be seen on X-ray. In cases where we are uncertain as to the extent of the damage to the tendon, though, an MRI scan may be necessary, which images the soft tissues better than X-rays. When the tendon is simply inflamed and not severely damaged, the problem may or may not be visible on MRI. It depends upon the severity of the condition.
Nonsurgical Treatment
Many physical therapies exist to help with the pain. We have found the combination of modalities, stretching, acupuncture, footwear modification and myofascial release to be very effective. In resilient cases, a promising new treatment called Radial Shockwave may be indicated. The key to the treatment of this, and other foot problems, is an accurate diagnosis. With this, a treatment regimen tailored to you and your specific situation can be devised. We treat many acute and chronic achilles tendinitis in Edmonton and St. Albert, so remember ?it shouldn?t hurt.?
Surgical Treatment
Following the MRI or ultrasound scan of the Achilles tendon the extent of the degenerative change would have been defined. The two main types of operation for Achilles tendinosis are either a stripping of the outer sheath (paratenon) and longitudinal incisions into the tendon (known as a debridement) or a major excision of large portions of the tendon, the defects thus created then being reconstructed using either allograft (donor tendon, such as Wright medical graft jacket) or more commonly using a flexor hallucis longus tendon transfer. In cases of Achilles tendonosis with more minor degrees of degenerative change the areas can be stimulated to repair itself by incising the tendon, in the line of the fibres, which stimulates an ingrowth of blood vessels and results in the healing response. With severe Achilles tendonosis, occasionally a large area of painful tendon needs to be excised which then produces a defect which requires filling. This is best done by transferring the flexor hallucis longus muscle belly and tendon, which lies adjacent to the Achilles tendon. This results in a composite/double tendon after the operation, with little deficit from the transferred tendon.
Prevention
Stay in good shape year-round and try to keep your muscles as strong as they can be. Strong, flexible muscles work more efficiently and put less stress on your tendon. Increase the intensity and length of your exercise sessions gradually. This is especially important if you've been inactive for a while or you're new to a sport. Always warm up before you go for a run or play a sport. If your muscles are tight, your Achilles tendons have to work harder to compensate. Stretch it out. Stretch your legs, especially your calves, hamstrings, quadriceps, and thigh muscles - these muscles help stabilize your knee while running. Get shoes that fit properly and are designed for your sport. If you're a jogger, go to a running specialty store and have a trained professional help you select shoes that match your foot type and offer plenty of support. Replace your shoes before they become worn out. Try to run on softer surfaces like grass, dirt trails, or synthetic tracks. Hard surfaces like concrete or asphalt can put extra pressure on the joints. Also avoid running up or down hills as much as possible. Vary your exercise routine. Work different muscle groups to keep yourself in good overall shape and keep individual muscles from getting overused. If you notice any symptoms of Achilles tendonitis, stop running or doing activities that put stress on your feet. Wait until all the pain is gone or you have been cleared to start participating again by a doctor.
What May Cause Pain At The Heel And Ways To Deal With It

Overview
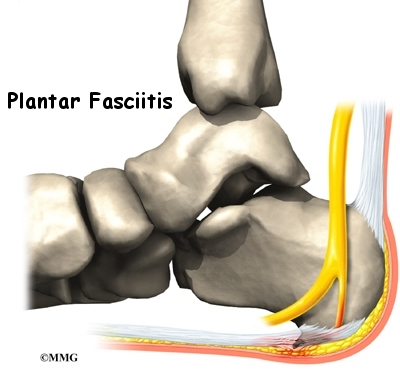
Plantar fasciitis is a common cause of heel pain in adults. The pain is usually caused by collagen degeneration (which is sometimes misnamed “chronic inflammation”) at the origin of the plantar fascia at the medial tubercle of the calcaneus. This degeneration is similar to the chronic necrosis of tendonosis, which features loss of collagen continuity, increases in ground substance (matrix of connective tissue) and vascularity, and the presence of fibro-blasts rather than the inflammatory cells usually seen with the acute inflammation of tendonitis. The cause of the degeneration is repetitive microtears of the plantar fascia that overcome the body's ability to repair itself.
Causes
Plantar fasciitis can develop when your feet roll in too far as you take each step. This rolling in, known as over-pronation, can happen for many reasons. It can be due to excessive weight gain, pregnancy, quickly increasing physical activity, tight calf muscles, poor biomechanics or merely wearing unsupportive, flat footwear. When your feet over-pronate, your arches can collapse, putting strain on the tissues in the bottom of your foot.
Symptoms
The major complaint of those with plantar fasciitis is pain and stiffness in the bottom of the heel. This develops gradually over time. It usually affects just one foot, but can affect both feet. Some people describe the pain as dull, while others experience a sharp pain, and some feel a burning or ache on the bottom of the foot extending outward from the heel. The pain is usually worse in the morning when you take your first steps out of bed, or if you’ve been sitting or lying down for a while. Climbing stairs can be very difficult due to the heel stiffness. After prolonged activity, the pain can flare-up due to increased inflammation. Pain is not usually felt during the activity, but rather just after stopping.
Diagnosis
Your doctor will ask you about the kind of pain you're having, when it occurs and how long you've had it. If you have pain in your heel when you stand up for the first time in the morning, you may have plantar fasciitis. Most people with plantar fasciitis say the pain is like a knife or a pin sticking into the bottom of the foot. After you've been standing for a while, the pain becomes more like a dull ache. If you sit down for any length of time, the sharp pain will come back when you stand up again.
Non Surgical Treatment
The good news is that plantar fasciitis is reversible and very successfully treated. About 90 percent of people with plantar fasciitis improve significantly within two months of initial treatment. If your plantar fasciitis continues after a few months of conservative treatment, your doctor may inject your heel with steroidal anti-inflammatory medications (corticosteroid). Cortisone injections have been shown to have short-term benefits but they actually retard your progress in the medium to long-term, which usually means that you will suffer recurrent bouts for longer. Due to poor foot biomechanics being the primary cause of your plantar fasciitis it is vital to thoroughly assess and correct your foot and leg biomechanics to prevent future plantar fasciitis episodes or the development of a heel spur. Your physiotherapist is an expert in foot assessment and its dynamic biomechanical correction. They may recommend that you seek the advice of a podiatrist, who is an expert in the prescription on passive foot devices such as orthotics.
Surgical Treatment
In unusual cases, surgical intervention is necessary for relief of pain. These should only be employed after non-surgical efforts have been used without relief. Generally, such surgical procedures may be completed on an outpatient basis in less than one hour, using local anesthesia or minimal sedation administrated by a trained anesthesiologist. In such cases, the surgeon may remove or release the injured and inflamed fascia, after a small incision is made in the heel. A surgical procedure may also be undertaken to remove bone spurs, sometimes as part of the same surgery addressing the damaged tissue. A cast may be used to immobilize the foot following surgery and crutches provided in order to allow greater mobility while keeping weight off the recovering foot during healing. After removal of the cast, several weeks of physical therapy can be used to speed recovery, reduce swelling and restore flexibility.
Prevention
The best way to prevent plantar fasciitis is to wear shoes that are well made and fit your feet. This is especially important when you exercise or walk a lot or stand for a long time on hard surfaces. Get new athletic shoes before your old shoes stop supporting and cushioning your feet. You should also avoid repeated jarring to the heel. Keep a healthy weight. Do your leg and foot stretching exercises regularly.
What Brings About Plantar Fasciitis

Overview
At the bottom of your foot there's a thick band of connective tissue called the plantar fascia or arch tendon. It connects your heel bone (calcaneus) to the front of your foot. If the plantar fascia becomes irritated and sore from overuse, it's known as plantar fasciitis. Plantar fasciitis sometimes can be mistaken for heel spurs, which is a different kind of injury with similar symptoms. Plantar fasciitis is a common cause of heel pain in runners, dancers, and athletes in sports that involve a lot of running or jumping. You don't have to be active to get plantar fasciitis. It can affect anyone. People who are overweight, pregnant women, people whose jobs involve a lot of standing, and people who wear worn-out shoes all have a higher chance of getting plantar fasciitis.
Causes
Plantar Fasciitis often leads to heel pain, heel spurs, and/or arch pain. The excessive stretching of the plantar fascia that leads to the inflammation and discomfort can be caused by the following: Over-pronation (flat feet) which results in the arch collapsing upon weight bearing A foot with an unusually high arch A sudden increase in physical activity Excessive weight on the foot, usually attributed to obesity or pregnancy Improperly fitting footwear Over-pronation (flat feet) is the leading cause of plantar fasciitis. Over-pronation occurs in the walking process, when a person's arch collapses upon weight bearing, causing the plantar fascia to be stretched away from the heel bone. With Plantar Fasciitis, the bottom of your foot usually hurts near the inside of the foot where the heel and arch meet. The pain is often acute either first thing in the morning or after a long rest, because while resting the plantar fascia contracts back to its original shape. As the day progresses and the plantar fascia continues to be stretched, the pain often subsides.
Symptoms
Among the symptoms for Plantar Fasciitis is pain usually felt on the underside of the heel, often most intense with the first steps after getting out of bed in the morning. It is commonly associated with long periods of weight bearing or sudden changes in weight bearing or activity. Plantar Fasciitis also called “policeman’s heel” is presented by a sharp stabbing pain at the bottom or front of the heel bone. In most cases, heel pain is more severe following periods of inactivity when getting up and then subsides, turning into a dull ache.
Diagnosis
After you describe your symptoms and discuss your concerns, your doctor will examine your foot. Your doctor will look for these signs. A high arch, an area of maximum tenderness on the bottom of your foot, just in front of your heel bone. Pain that gets worse when you flex your foot and the doctor pushes on the plantar fascia. The pain improves when you point your toes down. Limited "up" motion of your ankle. Your doctor may order imaging tests to help make sure your heel pain is caused by plantar fasciitis and not another problem. X-rays provide clear images of bones. They are useful in ruling out other causes of heel pain, such as fractures or arthritis. Heel spurs can be seen on an x-ray. Other imaging tests, such as magnetic resonance imaging (MRI) and ultrasound, are not routinely used to diagnose plantar fasciitis. They are rarely ordered. An MRI scan may be used if the heel pain is not relieved by initial treatment methods.
Non Surgical Treatment
Reducing inflammation in the plantar fascia ligament is an important part of treatment, though this does not address the underlying damage to the ligament. Initial home treatment includes staying off your feet and applying ice for 15 to 20 minutes three or four times a day to reduce swelling. You can also try reducing or changing your exercise activities. Using arch supports in your shoes and doing stretching exercises may also help to relieve pain. Nonsteroidal anti-inflammatory drugs (NSAIDS), such as ibuprofen (i.e. Motrin or Advil) and naproxen (i.e. Aleve), are often used to reduce inflammation in the ligament. If home treatments and over-the-counter anti-inflammatory drugs don’t ease the pain, an injection of a corticosteroid directly into the damaged section of the ligament can be given. Your doctor can do this in his or her office. Your doctor may use an ultrasound device to help determine the best place for the injection. Corticosteroids can also be administered on the skin of your heel or the arch of your foot, and then a painless electrical current is applied to let the steroid pass through your skin and into the muscle. Physical therapy is an important part of treatment for planter fasciitis. It can help stretch your plantar fascia and Achilles tendons. A physical therapist can also show you exercises to strengthen your lower leg muscles, helping to stabilize your walk and lessen the workload on your plantar fascia. If pain continues and other methods aren’t working, your doctor may recommend extracorporeal shock wave therapy. Sound waves are bombarded against your heel to stimulate healing within the ligament. This treatment can result in bruises, swelling, pain, and numbness, and has not been proven to be consistently effective in relieving symptoms.

Surgical Treatment
Surgery is usually not needed for plantar fasciitis. About 95 out of 100 people who have plantar fasciitis are able to relieve heel pain without surgery. Your doctor may consider surgery if non-surgical treatment has not helped and heel pain is restricting your daily activities. Some doctors feel that you should try non-surgical treatment for at least 6 months before you consider surgery. The main types of surgery for plantar fasciitis are Plantar fascia release. This procedure involves cutting part of the plantar fascia ligament . This releases the tension on the ligament and relieves inflammation . Other procedures, such as removing a heel spur or stretching or loosening specific foot nerves. These surgeries are usually done in combination with plantar fascia release when there is lasting heel pain and another heel problem. Experts in the past thought that heel spurs caused plantar fasciitis. Now experts generally believe that heel spurs are the result, not the cause, of plantar fasciitis. Many people with large heel spurs never have heel pain or plantar fasciitis. So surgery to remove heel spurs is rarely done.
Prevention
An important part of prevention is to perform a gait analysis to determine any biomechanical problems with the foot which may be causing the injury. This can be corrected with orthotic inserts into the shoes. If symptoms do not resolve then surgery is an option, however this is more common for patients with a rigid high arch where the plantar fascia has shortened.